

Frozen shoulder, likewise called cement capsulitis, is a condition that causes agony and firmness in the shoulder. After some time, one may think that it’s very difficult to move the shoulder. In any case, more often than not patients see that after a time of declining manifestations, the solidified shoulder will in general show signs of improvement, albeit full recuperation may take up to a couple of months. Exercise-based recuperation, which spotlights on improving shoulder portability, is the essential treatment suggestion. Frozen shoulder most regularly influences individuals between the ages of 40 and 60, and happens in ladies more frequently than men. Also, individuals with diabetes are at an expanded danger of building up a solidified shoulder.
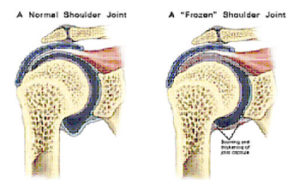
Your shoulder is organized like a ball-and-attachment. It is comprised of three bones: your upper arm bone (humerus), your shoulder bone (scapula), and your collarbone (clavicle).The humerus bone (ball) into a shallow attachment (glenoid) in your shoulder bone. The bones are held together by a Strong connective tissue, called the shoulder case, encompasses the joint. The container is typically flexible, permitting, boundaries of development in the shoulder. A grease called synovial liquid helps facilitate the developments.

In a solidified shoulder, the shoulder container thickens and turns out to be hardened and tight. Thick groups of tissue — called bonds — create. As a rule, there is less synovial liquid in the joint. The trademark indications of this condition are extreme torment and being not able to move your shoulder — either all alone or with the assistance of another person
It usually develops in three stages:
Stage 1: Freezing
In the “freezing” stage, you may experience progressively increasing pain. As the pain worsens, you may develop stiffness of the shoulder, ie; your shoulder loses range of motion. Freezing typically lasts from 6 weeks to 9 months.
Stage 2: Frozen
During this phase, pain subsides. However, stiffness persists and you will be unable to move your shoulder properly. Activities like lifting your arm, reaching your back, combing the hair and wearing your shirt becomes difficult/ impossible. During these 4 to 6 months, daily activities may be very difficult.
Stage 3: Thawing
Shoulder motion slowly improves during the “thawing” stage. Complete return to normal or close to normal strength and motion typically takes approximately 6-12 months.
The causes of frozen shoulder are not fully understood. Many times a clear cause cannot be established. There is no clear connection to arm dominance or occupation. A few factors may put you more at risk for developing frozen shoulder.
Diabetes. Frozen shoulder occurs much more often in people with diabetes. The reason for this is not known. In addition, diabetic patients with frozen shoulder tend to have a greater degree of stiffness that continues for a longer time before “thawing.”
Other diseases. Some additional medical problems associated with frozen shoulder include hypothyroidism, hyperthyroidism, Parkinson’s disease, and cardiac disease.
Immobilization. Frozen shoulder can develop after the shoulder has been immobilized for a period of time due to surgery, a fracture, or other injury. (Emphasis on early mobility exercises can help prevent frozen shoulder after a major surgery/ injury).
Pain from frozen shoulder is usually dull or aching. It is typically worse early in the course of the disease and when you move your arm. The pain is usually located over the outer shoulder area and sometimes the upper arm. As discussed earlier, you will find it difficult to perform activities of daily living like combing hair, wearing shirts, reaching the back.
Physical Examination
After discussing your symptoms and medical history, your doctor will examine your shoulder.
Your doctor will move your shoulder carefully in all directions to see if movement is limited and if pain occurs with the motion. The range of motion when someone else moves your shoulder is called “passive range of motion.” Your doctor will compare this to the range of motion you display when you move your shoulder on your own (“active range of motion”). People with frozen shoulder have limited range of motion both actively and passively.
Imaging Tests
Your surgeon may request other to rule out other causes of stiffness and pain.
X-rays: X-rays may show other problems in your shoulder, such as arthritis.
Magnetic resonance imaging (MRI) and ultrasound: These studies can create better images of soft tissues. They are not required to diagnose frozen shoulder, however, they may help to identify other problems in your shoulder, such as a torn rotator cuff.
Most patients with frozen shoulder generally gets better over time, although it may a few months. The focus of treatment is to control pain and restore motion and strength.
Nonsurgical Treatment
 Most people with frozen shoulder improve with relatively simple treatments to control pain and restore motion.
Most people with frozen shoulder improve with relatively simple treatments to control pain and restore motion.
Non-steroidal anti-inflammatory medicines to reduce pain and swelling.
Steroid injections. Cortisone is a powerful anti-inflammatory medicine that is injected directly into your shoulder joint.
Physical therapy: This is done under the supervision of a physical therapist. Specific exercises will help restore motion. Therapy includes stretching or range of motion exercises for the shoulder. Sometimes heat is used to help loosen the shoulder up before stretching. Below are examples of some of the exercises that might be recommended.
Surgical Treatment

If your symptoms are not relieved by therapy and anti-inflammatory medicines, you and your doctor may discuss surgery. It is important to talk with your doctor about your potential for recovery continuing with simple treatments, and the risks involved with surgery.
The goal of surgery for frozen shoulder is to stretch and release the stiffened joint capsule. The most common methods include manipulation under anesthesia and shoulder arthroscopy.
Manipulation under anesthesia. During this procedure, you are put to sleep. Your doctor will force your shoulder to move which causes the capsule and scar tissue to stretch or tear. This releases the tightening and increases range of motion.
Shoulder arthroscopy. In this procedure, your doctor will cut through tight portions of the joint capsule. This is done using pencil-sized instruments inserted through small incisions around your shoulder.
In many cases, manipulation and arthroscopy are used in combination to obtain maximum results. Most patients have very good outcomes with these procedures.
Recovery: After surgery, physical therapy is necessary to maintain the motion that was achieved with surgery. Recovery times vary, from 6 weeks to three months. Although it is a slow process, your commitment to therapy is the most important factor in returning to all the activities you enjoy.
Long-term outcomes after surgery are generally good, with most patients having reduced or no pain and greatly improved range of motion. In some cases, however, even after several years, the motion does not return completely and a small amount of stiffness remains.
Although uncommon, frozen shoulder can recur, especially if a contributing factor like diabetes is still present.